AI-Driven Segmentation on Weight Bearing CT Introduction Accurate segmentation is critical for orthopedic workflows, including…
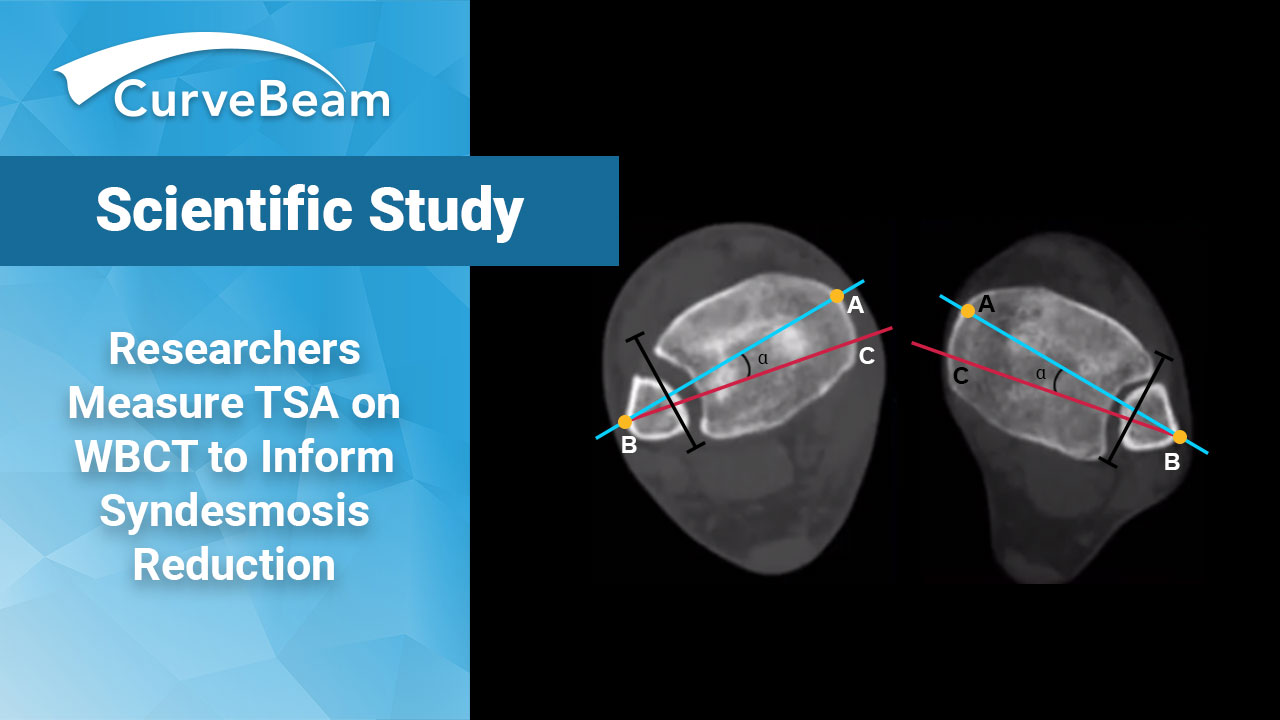
Researchers Measure TSA on WBCT to Inform Syndesmosis Reduction
Weight Bearing CT (WBCT) has been shown to be a reliable method to diagnose syndesmotic instability. Yet when it comes to syndesmosis reduction, a common concern for physicians is clamp mispositioning.
A team of researchers at Foot & Ankle Research and Innovation Laboratory (FARIL), a research lab at the Massachusetts General Hospital in Boston took a look at how WBCT imaging could help with improving syndsmosis reduction outcomes. They hypothesized that determining the trans-syndesmotic angle (TSA) using WBCT can not only help surgeons with placing the clamp more accurately, but can also help reduce the risk of malreduction.
Many authors have demonstrated the unreliability of (plain) radiographic assessment of syndesmotic reduction in the coronal and sagittal planes and have cautioned on the high rates of malreduction. – Putnam et al
To define reference values on WBCT, the researchers measured the TSA at 1 cm, 2 cm, and 3 cm proximal to the tibial plafond on weight bearing CT images of healthy individuals. It was found that all three TSA measurements were significantly different from the historically defined syndesmotic angle of 30 degrees. The mean TSA on WBCT was 17.6 at 1 cm; 21.6 at 2 cm; and 24.1 at 3 cm.
Based on these findings, they recommended the medial tine of the clamp should be positioned at 24.7% and 21.3% of the AP tibial cortical distance, posterior to the anterior tibial cortex at 1cm and 2cm proximal to the tibial plafond at 24.7.% and 21.3% of the AP tibial cortical distance, posterior to the anterior tibial cortex at 1cm and 2cm proximal to the tibial plafond.
Visit FARIL’s Instagram post for more here.
Related Posts