WBCT on the Program Thursday, January 22 11:10 am – 12:30 pm Symposium 2: Diagnostic…
Surgeons Weigh In: Top Indications for WBCT
Weight bearing CT (WBCT) imaging has fundamentally changed the evaluation and management of foot and ankle disorders such as hallux valgus, progressive collapsing foot disorder (PCFD), ankle instability, and traumatic deformities. The following panel of experts share their insights and experiences in the use of WBCT in clinical practice as well as their opinions on the future direction of the modality.
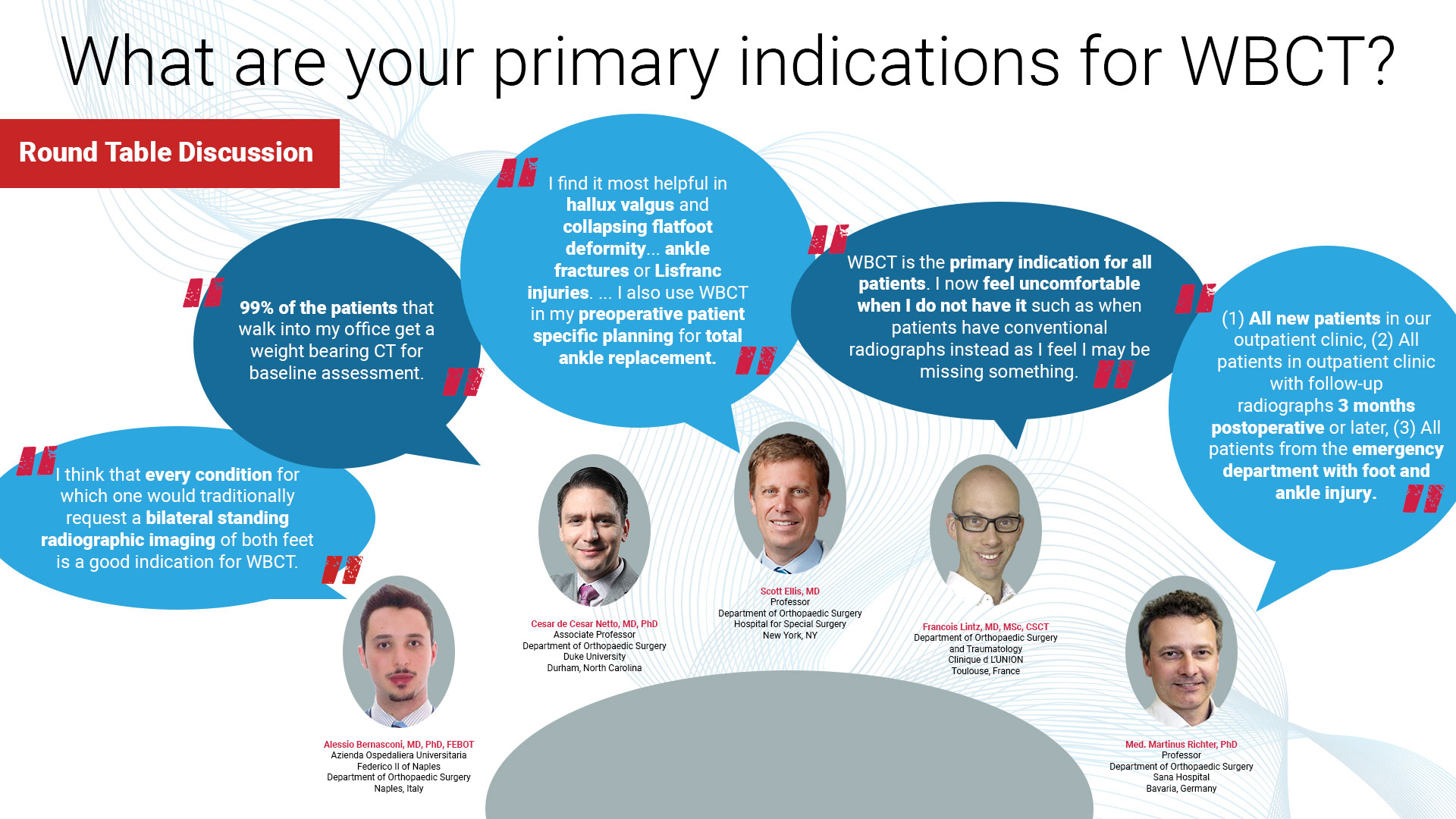
What are your primary indications for WBCT?

Dr. Alessio Bernasconi, MD, PhD, FEBOT
Azienda Ospedaliera Universitaria
Federico II of Naples
Department of Orthopaedic Surgery
Naples, Italy
I think that every condition for which one would traditionally request a bilateral standing radiographic imaging of both feet is a good indication for WBCT. Even soft tissue issues (i.e. plantar fasciitis or non insertional Achilles tendinopathy, ligamentous insufficiency) bring the physician to assess the foot alignment during stance in order to explain excessive strain on tendons and ligaments or to evaluate the structural consequences of potential instabilities. Dr. de Cesar Netto: I utilize weight bearing CT assessment for pretty much all my new patients. Unless the complaint is exclusively related to soft tissue problems such as a plantar fashion nodule, for example, or other issues that could be completely independent from malalignment scenarios, which are rare. So basically, 99% of the patients that walk into my office get a weight bearing CT for baseline assessment. Obviously, there are some pathologies where the weight bearing CT is mandatory in my opinion, such as assessment of progressive collapsing foot deformity, cavovarus deformity, hallux valgus, hallux rigidus, midfoot arthritis, ankle arthritis, and ankle instability.
I generally order a WBCT for 5 different conditions. I tend to use the technology in cases where I need to see the effect of weightbearing in three dimensions, particularly with deformity or instability. I find it most helpful in hallux valgus and collapsing flatfoot deformity. I also obtain the scan for ankle fractures or Lisfranc injuries, particularly when I would like to assess instability or diastases that might drive surgical treatment. I also use WBCT in my preoperative patient specific planning for total ankle replacement. Finally, I have found some use when looking at metatarsalgia or forefoot metatarsal balance.

Dr. Scott Ellis, MD
Professor
Department of Orthopaedic Surgery
Hospital for Special Surgery
New York, NY

Dr. Francois Lintz, MD, MSc, CSCT
Department of Orthopaedic Surgery
and Traumatology
Clinique d L’UNION
Toulouse, France
Cone Beam weightbearing CT is technologically a revolving radiographic setup: it’s effectively a 3D radiograph. Therefore, its indications are the same as radiographs. You just get a CT as a bonus, without extra radiation, and it is much faster. I no longer refer patients for radiographs or conventional CT in any case. WBCT is the primary indication for all patients. I now feel uncomfortable when I do not have it such as when patients have conventional radiographs instead as I feel I may be missing something.
Our indications are: (1) All new patients in our outpatient clinic, (2) All patients in outpatient clinic with follow-up radiographs 3 months postoperative or later, (3) All patients from the emergency department with foot and ankle injury, when weight bearing is not possible without weight bearing and optionally in lying position with HiRise device. From 2013 until present, we have performed more than 21,000 3D scans with pedCAT/HiRise for foot and ankle.

Dr. Martinus Richter, PhD
Professor
Department of Orthopaedic Surgery
Sana Hospital
Bavaria, Germany
To read the full roundtable discussion visit https://journals.sagepub.com/doi/10.1177/19386400241238608
Related Posts