Orthopedic decision-making depends on accurate representation of anatomy—particularly when joint alignment and bone relationships change…
WBCT – “New Gold Standard” for HV Pronation Measurements
Key Points
- A study from Hospital for Special Surgery found there is no correlation between 1st metatarsal pronation measured on weight bearing radiographs and 1st metatarsal pronation measured on weight bearing CT (WBCT).
- Researchers said WBCT should be considered the ”gold standard” for adequately measuring 1st metatarsal pronation in hallux valgus patients.
- One limitation of the study was that CAD modeling on WBCT scans was time consuming, but new softwares such as CubeVue Autometrics (investigational only; not available for sale) promise to automate this function.
First metatarsal pronation is increasingly recognized as an important aspect of hallux valgus (HV). Current standard of care involves obtaining weight bearing radiographs (WBXR).
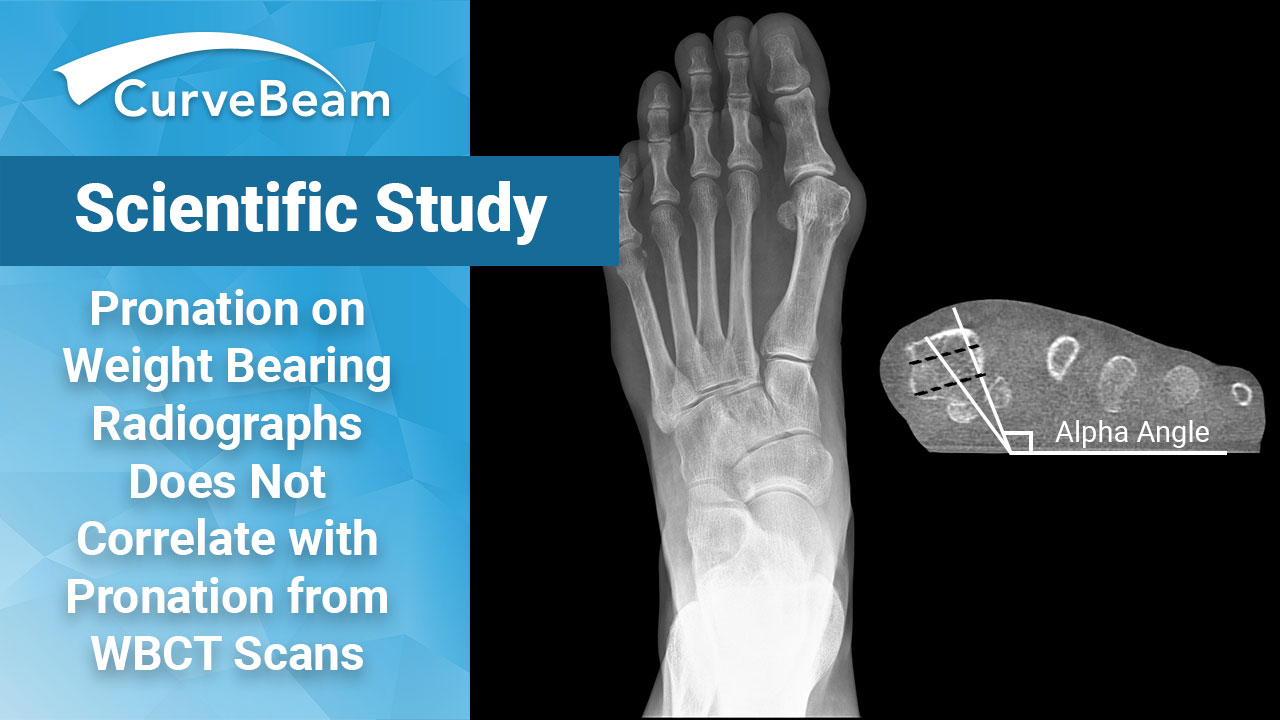
A recent study from the Hospital for Special Surgery in New York, however, suggests that the supplemental information obtained from the third dimension in weight bearing CT (WBCT) scans is essential for appropriately measuring 1st metatarsal pronation. Furthermore, the study concluded that pronation measurements on WBXR were weakly associated at best with pronation measurements on WBCT. Therefore, pronation measured on WBXR is not a substitute for pronation measured on WBCT, researchers said.
“WBCT scans should be considered a new gold standard for adequately measuring 1st metatarsal pronation in patients with HV,” – Patel et al, Foot Ank Surg
The study, by Dr. Tamanna J. Patel et al, was published in the October 2021 issue of Foot and Ankle Surgery.
HV is a 3-dimensional deformity that occurs in the coronal, sagittal, and axial planes. Due to the complexity and multiplanar views required, the limitations of WBXR are restricting. While studies exist individually for both WBXR and WBCT in reference to methods proposed to measure pronation of the 1st metatarsal, the main purpose of this study was to compare the two methods of measurement.
Materials and Methods
The study compared 29 patient datasets who fit the criteria of both having pre-operative and 5-month post-operative WBCT scans as well as corresponding WBXR of the affected foot.
Weight Bearing radiograph measurements were obtained from the AP view. Measurements included intermetatarsal angle (IMA) and the HV angle (HVA). The method described by Wagner and Wagner was used to measure pronation by examining the shape of the head of the 1st metatarsal. Patients were divided into one of four categories based on 1st metatarsal pronation: <9.9 degrees, 10.0 – 19.9 degrees, 20.0-29.9 degrees, and 30. Then Meary’s Angle was calculated using a lateral view.
WBCT measurements were obtained using two methods: the alpha angle (an angle formed by line that connects the crista and the dorsal center of the 1st metatarsal and the line vertical to the ground) as well as with the CAD modeling technique. Based on the alpha angle, patients were grouped in to the same four categories as described in the WBXR pronation measurements. Once the CAD modeling technique was performed, the models were uploaded to Geomagic Studio 2014. Using this software, an examiner picked landmarks on the cortex of the 1st metatarsal and 2nd metatarsal and utilized MATLAB 2019a to calculate the difference in rotation between the points on the 1st and 2nd metatarsal which defined 1st metatarsal pronation. These measurements were similarly placed into the four categories as described.
To determine if there was absolute agreement between the WBCT and radiographic scans pronation measurements, each alpha angle and CAD measurement on WBCT scan was placed into one of the four radiographic pronation groups described above. The same process was used to compare 3D CAD measurements with radiographic pronation pre- and post-operatively. Association between the radiographic pronation groups and the measurements of pronation on WBCT scans was determined using Spearman correlation coefficients. Finally, after dividing patients into plain radiograph pronation groups, differences in mean WBCT pronation of the 1st metatarsal using the alpha angle and CAD technique between the different radiographic pronation groups were compared using one-way ANOVA and post-hoc Tukey tests.
Conclusion
Agreement between the two observers’ pronation on WBXR was good (k = 0.634) and moderate (k = 0.501), retrospectively. There was no correlation between radiographic pronation and the 3D CAD model. Preoperatively, there was weak correlation between the alpha angle and the radiographic pronation groups, although this relationship did not hold postoperatively. There was also no difference in mean pronation calculated on WBCT scans between the plain radiographic groups.
Researchers concluded that pronation of the 1st metatarsal measured on WBXR had moderate interobserver agreement and was only weakly associated with pronation measured from WBCT scans. The results suggested that 1st metatarsal pronation measured on WBXR is not a substitute for pronation measured on WBCT scans.
It was noted that the study had important limitations, including the significant processing time of the CAD modeling method. The introduction of software such as CurveBeam’s Autometrics “will perform automatic…segmentation of bones and may allow for the measurement of the 1st metatarsal pronation to be calculated more quickly in the future,” researchers said.
Autometrics is investigational only and is not available for sale in the United States.
To read the full study please click here.
Related Posts