AI-Driven Segmentation on Weight Bearing CT Introduction Accurate segmentation is critical for orthopedic workflows, including…
Comparative Analysis of Structural Differences in Progressive Collapsing Foot Deformity With and Without Hallux Valgus
Key Points:
- Weight Bearing CT (WBCT) helps visualize several structural and alignment differences between Progressive Collapsing Foot Deformity (PCFD) with and without Hallux Valgus (HV).
- Rotation of the first tarsometatarsal joint, and intrinsic rotation of the first metatarsal bone were all associated with HV deformity.
- Semi-automatic measurement tools, such as CurveBeam AI’s TALAS* tool, can simplify and help more accurately diagnose foot deformities.
PCFD and HV are complex 3D foot deformities that share certain morphologic similarities, though the relationship between them hasn’t been extensively discussed for how common they are. The relationship between hindfoot and forefoot deformities has become increasingly evident with the introduction of WBCT.
Dr Cesar de Cesar Netto, MD, PhD, et. al out of the Division of Foot and Ankle Surgery, Department of Orthopaedic Surgery at Duke University School of Medicine in Durham, North Carolina aimed to investigate structural and alignment differences between PCFD with and without HV using WBCT. Researchers hypothesized that there were distinct hindfoot or midfoot structural or alignment variances between PCFD with and without HV deformities.
Method
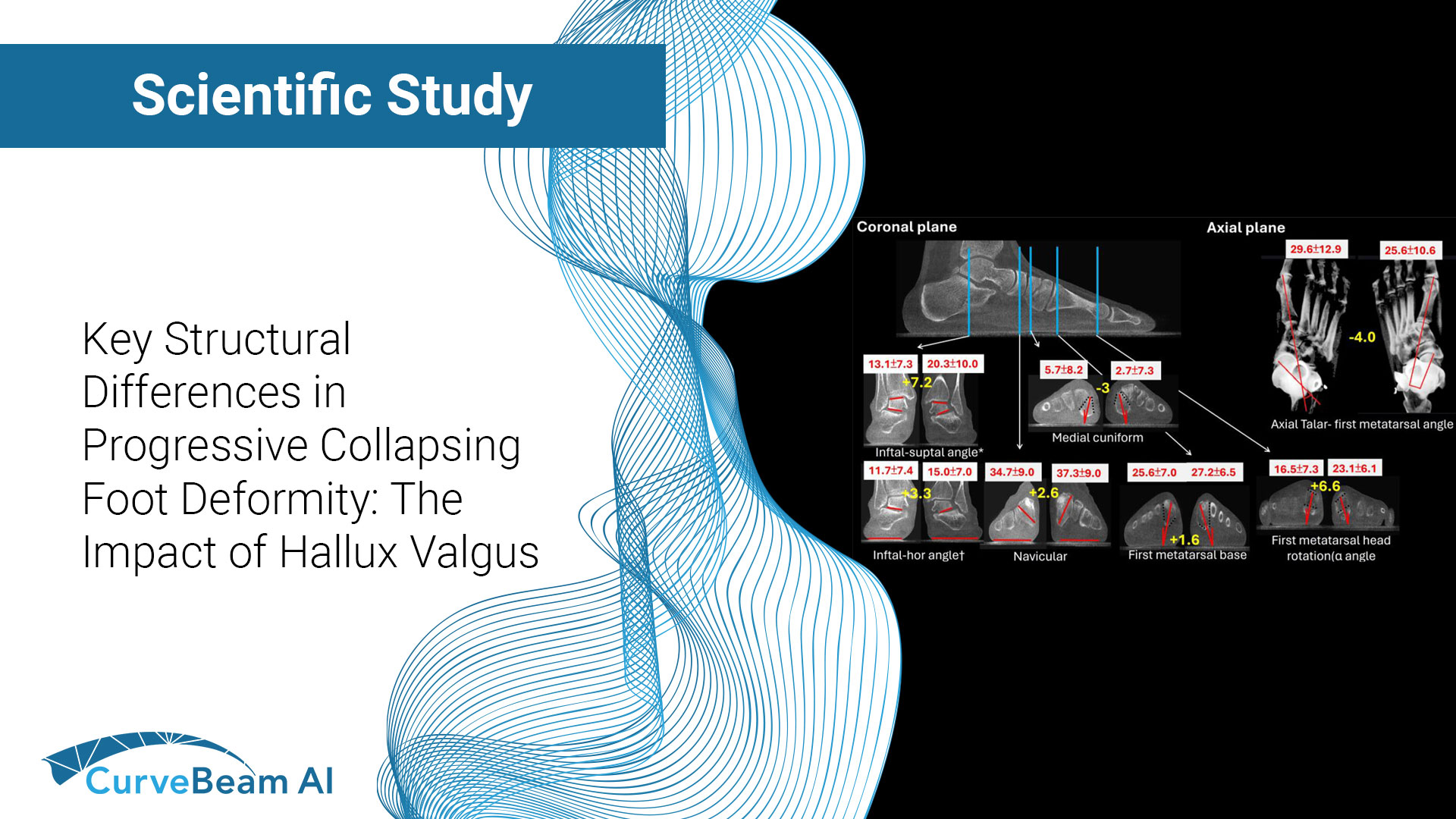
This retroactive analysis study included patients who were 18 years or older who were clinically diagnosed with PCFD and underwent WBCT (CurveBeam AI’s pedCAT or HiRise systems). Standard 2D PCFD and HV parameters were assessed utilizing CurveBeam AI’s semiautomatic Torque Ankle Lever Arm System (TALAS)* system. Foot and ankle offset, forefoot ach angle, and pronation of the medial column bones in the coronal plane, with the ground as a reference, were manually measured. The angles from the inferior aspect of subtalar posterior facet of the talus to the ground (subtalar horizontal angle), from the inferior (posterior facet) to superior facets of the talus (infratalar-supratalar angle), and from the inferior (posterior facet) of the talus to the superior facet of the calcaneus (infratalar-supracalcaneal angle) were also examined. HV was defined by an HV angle of greater than or equal to 15 degrees.
Results
Among the 72 feet studied, 33 displayed HV, whereas 39 did not. Researchers found that in the coronal plane, the PCFD with HV group showed a higher infratalar-supratalar angle and greater pronation at the first tarsometatarsal joint, first metatarsal bone, and head. The PCFD with HV group also exhibited greater naviculocuneiform joint supination. Generalized estimating equation logistic regression analysis revealed significant associations of HV deformity with the intrinsic rotation of the first metatarsal bone, infratralar-supratalar angle, and rotation of the first tarsometatarsal joint.
Conclusion
This study revealed significant differences between PFCD with and without HV deformity over several parameters, notably the infratalar-supratalar angle, rotation of the first tarsometatarsal joint, and intrinsic rotation of the first metatarsal bone were all associated with HV deformity.
Researchers hope that this study can serve as a foundation for future prospective longitudinal studies or dynamic research to further explore the relationships between PCFD and HV.
To read the full study click here.
*TALAS is investigational only and is not available for sale.
Images courtesy of Dr. Cesar de Cesar Netto.
Related Posts